Cardiologists also perform echocardiographies (cardiac ultrasound) as well. For the remaining portion of the week, we followed a couple of them and learned much about the use of ultrasound in evaluating a variety of patients. In the spirit of learning new imaging modalities this week, I will dedicate this post to the use of ultrasound to non-invasively determine heart conditions.
The appearance of cardiac anatomy when using ultrasound can be confusing. It is difficult to visualize a 3D construct utilizing 2D images. Courtesy of http://www.cpdsolutions.co.za/Publications/article_uploads/Cardiology_ultrasound.pdf, I hope this provides you with a baseline picture of cardiac ultrasound anatomy in general:

Cardiac ultrasound consists of using image planes about an axis to provide structure and sonographic shapes that relate to its 3D configuration. Dr. Huang and the other cardiologists have a unique, systematic approach to performing echocardiography, although there are many similarities. Here are some common echocardiography windows (courtesy of http://www.cpdsolutions.co.za/Publications/article_uploads/Cardiology_ultrasound.pdf):


The first view to orient oneself and to generally visualize the heart is called the long-axis parasternal view. In this view, left ventricle (LV) size change can be seen during systole and diastole as well as opening and closing of mitral and aortic valves. It is very useful in determining if mitral regurgitation, mitral valve prolapse, and aortic regurgitation is present.
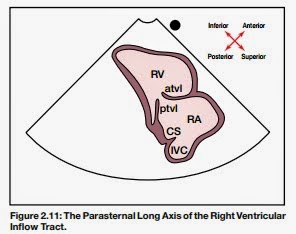

The second view is the long axis parasternal right ventricular inflow tract view. Tricuspid valves can be visualized and whether or not tricuspid regurgitation is seen.

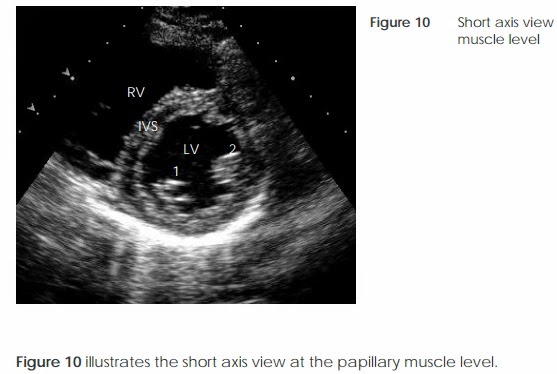
The following views demonstrate a short-axis parasternal view (imagine the transducer perpendicular to the long axis view) at various heart region levels - one at the mitral valve and the latter at the left ventricular papillary muscle. These views are ideal for looking at structural contractile motion (i.e. aortic valves, mitral valve, ventricular and atrial wall motion) and identifying VSD, ASD, and PDA.


The next view is the subxiphoid apical view of either four or five chambers. This is probably the easiest to visualize with the transducer looking at the heart apex closest. It is also one of the most powerful as you can assess contractile function, study the heart valves, and delineate calcifications, lesions, and pericardial effusion. Regurgitation flow patterns can also be reinforced in this view. LV ejection faction using the Simpson Method (3D approximation using a 2D derivative base interval) can be calculated by determining the end-diastolic and end-systolic LV frames.


This view is similar to the four/five chamber apical view, but only shows three chambers. Courtesy of: http://123sonography.com/node/753 and http://webservice1.mvm.ed.ac.uk/imaging/demo/images/basic_echo_3chamber_scan.jpg, a lot of abnormalities can be determined. Aneurysms, abnormal wall motion, clot formation, pericardial effusion, and mitral valve integrity can be evaluated.


The last view to this systematic approach is the sub coastal vena cava view. Courtesy of: http://cardiophile.org/wp-content/uploads/2009/09/PAH-subcostal-IVC.jpg and http://123sonography.com/node/754, the IVC can be visualized as demonstrated with one of the three hepatic veins merging into the IVC, which eventually directs into the RA. Consequently, the IVC diameter can be determined. One of the unique aspects of using this view is that since there is no bone or lung tissue to obstruct the view of the heart, the sub coastal window can substitute for other windows if echogenicity is not reliable.
In addition to these views, ultrasound allows us to to not only perform 2D imaging, but also M-mode and Doppler imaging as well. M-mode echo is a 1D view that can be used to determine a multitude of things such as LVEF and heart structure sizes. This is due to the fact that temporal and spatial resolutions are much higher since the focus is only one of the lines from the 2D trace. Doppler imaging is an enhanced form of echo in which blood-flow velocity can be estimated by determining the frequency change of transmitted and reflected sound waves. Color-flow mapping is one type of doppler measurement that can be used to determine velocity and direction of blood flow. This is very useful in determining abnormal heart chamber flow and can guide a clinician towards a regurgitation or septal defect. Pulsed-wave doppler is another modality that was used by the doctors here, which makes localized velocity measurements in a small area at a specified tissue depth. The interesting part is that pressure gradients can be determined and is used primarily for quantification of pulmonary hypertension by estimating at the tricuspid valve level. Similarly, heart sounds can be recorded using this same technology at any of the valve levels.
Personal Note: In the right hands, ultrasound can be a very powerful tool in determining a specific heart condition accurately. However, it is very prone to operator error. During my time in the ultrasound room, each doctor had their own style to using ultrasound. It was easy to delineate those who had decades of experience as they were very comfortable with using it and at the same time, talking to the patient and generating a complete report. Even after a couple of days immersing myself in all things ultrasound, I am still a novice in distinguishing minute details that would change a clinical diagnosis especially in color-flow mapping. I am humbled in the face of these experienced practitioners.
Dr. Huang also discussed a bit about the medical system in Taiwan. Unlike in the US, where high school students are required to graduate with a college degree prior to matriculating into a medical school, in Taiwan, students can go directly into medical school if their grades are good. This means that there is very high level of Taiwanese medical students compared to other countries. Due to the early age in matriculation, he believes that many students become impatient and would rather go into relatively better compensated specialties. In this case, there is a growing shortage of primary care physicians in Taiwan. However, since many academically accomplished students go into medical school, their education is top tier (even more so when compared to other technical careers such as engineering and law). He implied that might also be one of the reasons why laws here are really as enforced compared to the US besides the past political suppression/viewpoints.
No comments:
Post a Comment